IGF-1 LR3 Before and After: Research Results, Timeline and Real Effects

This article is intended for educational and research purposes only. IGF-1 LR3 is not FDA-approved for bodybuilding, anti-aging, or general wellness use. All protocols referenced are from published research or supervised clinical settings. Consult a qualified healthcare provider before considering any peptide therapy. WADA and most major athletic organizations ban this compound.
The topic of IGF-1 LR3 Before and After has become increasingly popular in peptide and growth factor research. Scientists study this synthetic peptide to understand better its interactions with cellular growth signaling pathways, muscle tissue development, and metabolic regulation. Because insulin-like growth factor compounds play a critical role in biological growth processes, modified analogs such as IGF-1 LR3 provide valuable tools for investigating cellular development and regeneration.
IGF-1 LR3 is an advanced form of the insulin-like growth factor peptide that has been engineered with structural modifications to extend its half-life and enhance biological activity. These changes allow researchers to observe sustained receptor activation and analyze how growth factor signaling influences protein synthesis and tissue repair mechanisms. Studies examining IGF-1 LR3 before and after results help laboratories evaluate changes in cell proliferation, muscle biology, and metabolic signaling pathways.
What Is IGF-1 LR3?
If you’ve been researching peptide therapy, performance recovery, or anti-aging protocols, you’ve almost certainly come across IGF-1 LR3. But there’s persistent confusion about what it actually is and, more importantly, what realistic before-and-after results look like based on current research.
Let’s start with the science, because it matters enormously for understanding the timeline and effects.
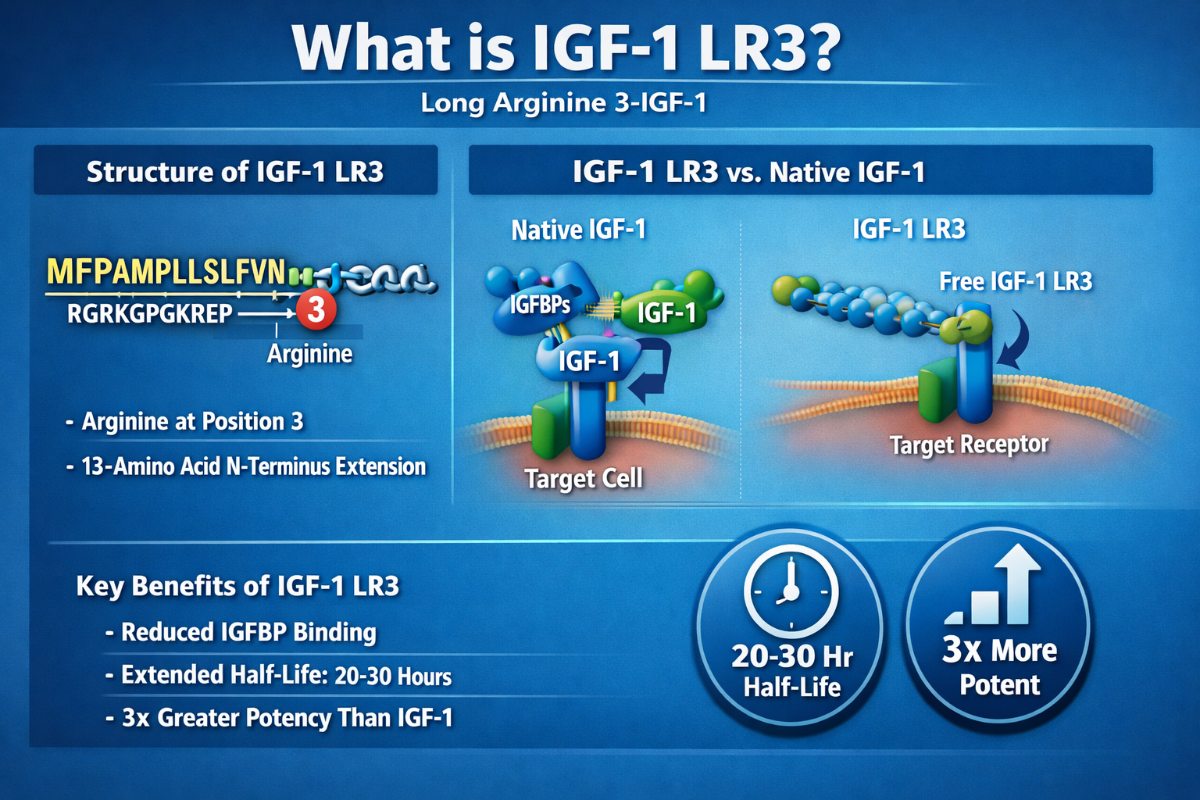
IGF-1 LR3 (Long Arginine 3-IGF-1) is a synthetic 83-amino acid analog of human Insulin-Like Growth Factor-1. The “LR3” designation refers to two structural modifications that make it fundamentally different from endogenous IGF-1:
- Arginine substitution: An arginine replaces glutamic acid at position 3 in the amino acid sequence
- 13-amino acid N-terminus extension: The sequence MFPAMPLLSLFVN is added at the front of the molecule
These aren’t cosmetic changes. They completely transform the compound’s behavior in the body. If you’re new to researching peptides broadly, our complete guide to the best peptides for research provides a useful foundation before diving deeper into specific analogs.
Native IGF-1 is rapidly neutralized by Insulin-Like Growth Factor Binding Proteins (IGFBPs), which act as gatekeepers controlling how much IGF-1 reaches cellular receptors. The LR3 modification dramatically reduces IGFBP binding affinity, allowing the molecule to circulate freely and interact directly with IGF-1 receptors (IGF-1R) on target cells.
The result a half-life of 20-30 hours compared to IGF-1’s 12–15 hours, and potency estimated to be approximately 3x greater than native IGF-1.
The Molecular Mechanism: What Actually Happens at the Cellular Level
Understanding the before-and-after narrative requires understanding what IGF-1 LR3 does on a cellular level. This isn’t abstract biology it directly explains the timeline of observable effects. When IGF-1 LR3 binds to the IGF-1 receptor, it initiates the PI3K/Akt/mTOR signaling pathway one of the master regulatory systems for cellular growth, survival, and metabolism.
Anabolic signaling cascade:
- mTOR activation → increases protein synthesis rate
- Satellite cell stimulation → activates dormant muscle stem cells to proliferate and fuse into existing muscle fibers
- MyoD protein activation → drives muscle hypertrophy at the transcriptional level
- FOXO pathway inhibition → reduces muscle protein breakdown (anti-catabolic effect)
Metabolic effects:
- Enhanced glucose uptake into muscle and adipose cells via GLUT-4 transporter upregulation
- Improved amino acid shuttling into cells, increasing substrate availability for tissue repair
- Myostatin inhibition reduces the body’s natural “brake” on muscle growth
- Lipolytic signaling encourages fat mobilization, contributing to body recomposition
Tissue repair and regeneration:
- Collagen synthesis stimulation relevant for tendons, ligaments, and connective tissue repair
- Nerve regeneration support via neurotrophin-like activity
- Satellite cell recruitment particularly important for recovery from training stress or injury
This multi pathway activity is why IGF-1 LR3 consistently ranks among the top compounds in our research on the best peptides for muscle growth, attracting attention across bodybuilding recovery, regenerative medicine, anti-aging protocols and injury rehabilitation research.
IGF-1 LR3 Before and After: The Realistic Timeline
One of the most common sources of misinformation online is the timeline. People either expect an overnight transformation or give up too early. Here’s what the research and supervised clinical experience actually show.
Phase 1: Hours 1–72 Invisible Foundation
The first effects are entirely subcellular. Within minutes of administration, IGF-1 LR3 binds to IGF-1 receptors and initiates the PI3K/Akt cascade. You won’t feel or see anything, but:
- Glucose and amino acid transport into cells increases
- Protein synthesis machinery is upregulated
- Anti-catabolic signaling begins to suppress muscle breakdown
This is the “laying the foundation” phase. Nothing visible happens, but the most critical molecular work is underway.
Phase 2: Days 3–14 Early Subjective Changes
Most research subjects and supervised users begin noticing the first subjective changes in this window:
- Improved muscle fullness cells are retaining more glycogen and water, creating a “pumped” appearance
- Faster workout recovery reduced delayed onset muscle soreness (DOMS), ability to train with greater frequency
- Increased training capacity subtle improvements in endurance and work output
- Sleep quality changes some users report deeper sleep, consistent with increased GH axis activity
- Mild water retention particularly around joints, which can also temporarily ease joint discomfort
These early changes are real but modest. The dramatic before-and-after transformations circulating online are almost always the result of 6–8+ week protocols combined with optimized nutrition and training not solo compound effects.
Phase 3: Weeks 2–4 Measurable Body Composition Shifts
This is where quantifiable changes begin to appear in research protocols. Body composition analysis (DEXA scan, bioimpedance, skinfold calipers) starts showing:
- Lean muscle mass gains progressive increases in muscle cross-sectional area, particularly in trained muscle groups
- Reduction in body fat percentage especially visceral and subcutaneous abdominal fat
- Strength improvements correlate with increased muscle fiber density and satellite cell incorporation
- Connective tissue adaptation tendon and ligament strengthening, reducing injury risk with progressive training loads
IGF-1 LR3’s dual anabolic and lipolytic properties make this phase particularly notable for body recomposition simultaneously building muscle while reducing fat a difficult feat to achieve through training and nutrition alone.
Phase 4: Weeks 4–8 Peak Effects and the Desensitization Warning
Research consistently identifies weeks 4–6 as the peak effectiveness window. This is when cumulative cellular changes more muscle satellite cells recruited, more mitochondria per cell, greater collagen density become most pronounced.
Critical Warning: After 4–6 weeks of daily use, IGF-1 receptors begin to downregulate. The cellular machinery becomes less responsive, diminishing returns set in, and the risk-to-benefit ratio shifts unfavorably. This is not a theoretical concern it is a documented pharmacological phenomenon with significant implications for protocol design.
Most well-designed research protocols use a 4-week-on/4-week-off cycling schedule. Some extend to 6 weeks, always followed by at least an equal rest period to allow full restoration of receptor sensitivity.
What Happens After the Cycle Ends
Post-cycle, the primary concern is maintaining gains while endogenous IGF-1 and growth hormone signaling normalize. Key considerations:
- Muscle gains made during the cycle are largely retained if training and nutrition remain consistent.
- The receptor downregulation reverses during the off period.
- Some researchers incorporate a post-cycle support protocol using growth hormone secretagogues to maintain GH axis activity during the rest window (see the comparison section below for relevant compounds)
Before and After: Specific Outcome Areas

Muscle Growth and Hypertrophy
Before: Individuals with plateaued muscle development despite consistent training and adequate protein intake often due to a ceiling on endogenous IGF-1 signaling capacity.
After (4–8 weeks, supervised protocol): Research data and supervised clinical outcomes show:
- Increases in lean muscle mass, particularly in trained muscle groups
- Enhanced muscle fiber density (both hypertrophy of existing fibers and hyperplasia of new fibers via satellite cell activation)
- Greater nitrogen retention is the biochemical indicator of a net anabolic state.
- Improved muscle vascularity due to increased capillarization of muscle tissue
The distinguishing feature compared to other anabolic interventions is the hyperplastic component IGF-1 LR3 doesn’t just make existing muscle cells bigger, it recruits new satellite cells that can become new muscle fibers. This is a meaningful mechanistic distinction, and a core reason it consistently ranks highly when comparing the best peptides for muscle growth side by side.
Fat Loss and Body Recomposition
Before: Individuals with stubborn fat deposits particularly visceral fat and lower abdominal fat who are resistant to dietary and exercise interventions.
After: IGF-1 LR3’s enhanced glucose disposal and lipolytic effects contribute to:
- Reduced fat storage in insulin-sensitive tissues
- Improved glucose uptake into muscle rather than fat cells
- A shift in substrate oxidation toward fat utilization
- The “leaning effect” commonly described — reduced body fat percentage with preserved or increased muscle mass
IGF-1 LR3 is not a standalone weight loss compound. Its fat loss effects are most pronounced in the context of a structured training program and appropriate caloric intake. Researchers studying metabolic outcomes alongside body composition sometimes pair it with GLP-1 receptor agonist analogs compounds like Tirzepatide 10mg and Retatrutide 10mg represent a distinct class targeting metabolic pathways rather than the IGF-1 axis, making the mechanistic comparison instructive.
Recovery and Injury Rehabilitation
This is arguably where the most compelling research exists. IGF-1 LR3’s effects on collagen synthesis, satellite cell activation, and connective tissue remodeling make it highly relevant for:
- Post-surgical rehabilitation (particularly orthopedic procedures)
- Tendon and ligament injury recovery
- Muscle strain and contusion healing acceleration
- Reducing recovery time between training sessions
Animal model research published in peer-reviewed journals demonstrates that direct injection of IGF-1 analogs significantly enhances muscle healing in lacerated, contused, and strain-injured muscles. Human clinical data, while more limited, are consistent with this mechanistic picture.
Skin Quality and Anti-Aging Applications
The anti-aging and aesthetic medicine interest in IGF-1 LR3 centers on its role in collagen and elastin synthesis, cellular regeneration, and skin tissue repair. Research subjects and clinical patients report:
- Improved skin elasticity and texture
- Reduced appearance of fine lines, particularly in sun-damaged skin
- Improved wound healing speed and quality
- Hair and nail quality improvements (via similar growth factor pathways)
This area is growing rapidly in aesthetic medicine and sits naturally alongside broader anti-aging peptide research. For context on the full anti-aging peptide landscape, our Best Peptides 2026 guide covers how IGF-1 LR3 compares against compounds like GHK-Cu, TB-500, and epithalon in regenerative and longevity applications.
Dosage, Administration, and Cycling Protocols
The following information is based on published research protocols and supervised clinical practice. IGF-1 LR3 dosing should only be undertaken under physician supervision. Self-administration carries significant risks, including hypoglycemia.
Research-Based Dosage Ranges
| Population | Typical Daily Dose | Frequency | Cycle Length |
|---|---|---|---|
| Research (Conservative) | 20–40 mcg | Once daily | 4–6 weeks |
| Research (Moderate) | 50–100 mcg | Once daily | 4 weeks |
| Clinical (Supervised) | Individualized | Per protocol | 4 weeks on / 4 weeks off |
Men: Supervised protocols typically use 40–50 mcg/day.
Women: Lower doses are generally appropriate, typically around 20 mcg per day.
Maximum: Most protocols cap at 100 mcg/day – doses above this significantly increase side effect risk with diminishing additional benefit
Timing Considerations
- Post-workout administration is most common, aligning with the natural window when IGF-1 receptors on muscle cells are most sensitive.
- Avoid administration within 2 hours of bedtime – may suppress endogenous growth hormone pulse.
- Do not administer in a fasted state without glucose monitoring – risk of hypoglycemia is highest when blood sugar is low.
- Morning doses on non-training days should be taken with a meal.
Reconstitution and Dosage Calculation
Lyophilized IGF-1 LR3 powder must be reconstituted with bacteriostatic water before use. Accurate reconstitution is critical – errors in calculation affect both efficacy and safety. Our Peptide Reconstitution Calculator provides instant, precise calculations for any peptide amount and dilution volume, eliminating common manual errors in research settings.
Administration Route
Subcutaneous (subQ) injection is standard in both research and supervised clinical settings. Intramuscular (IM) injection is used in some protocols. Oral bioavailability is negligible – any oral or “peptide spray” product claiming IGF-1 LR3 activity via non-injectable routes is not credible.
The Cycling Imperative
This cannot be overstated cycling is not optional it is pharmacologically necessary. IGF-1 receptor downregulation after 4–6 weeks of continuous use means that continuing beyond this window increases risk without proportional benefit. The minimum rest period equals the cycle length. Most experienced practitioners use a 4 weeks on/4 weeks off schedule as the standard protocol.
Risks, Side Effects, and Contraindications
Honest coverage of IGF-1 LR3 before-and-after results requires full transparency about the risks. This compound has a well-documented risk profile.
Primary Side Effects
Hypoglycemia (most important), IGF-1 LR3 enhances glucose uptake into cells, which can cause blood sugar to drop dangerously low. This is the most acutely dangerous side effect. Symptoms include shakiness, sweating, confusion, dizziness, and in severe cases, loss of consciousness. Glucose monitoring is essential, particularly in early cycles.
Insulin Resistance (with prolonged use) Paradoxically, while IGF-1 LR3 acutely improves glucose uptake, chronic high-dose use can promote insulin resistance as a compensatory mechanism. This is one reason cycling protocols were developed.
Fluid Retention: Mild water retention is common, particularly in early cycles. It is generally temporary and resolves within days of stopping. It can contribute to temporarily elevated blood pressure.
Receptor Desensitization As discussed, prolonged use reduces IGF-1 receptor sensitivity, creating diminishing returns and necessitating cycling.
Acromegaly-like Changes (supraphysiological doses). At very high doses (100+ mcg/day) for extended periods, jaw growth, brow changes, and enlarged extremities are genuine long-term concerns. At standard doses of 20–50 mcg for 4–6 week cycles, this risk is considered minimal.
Potential Oncogenic Risk Because IGF-1 LR3 stimulates cellular proliferation via pathways also implicated in tumor progression, individuals with personal or family history of cancer, or with precancerous conditions, face meaningful contraindications. Medical screening is non-negotiable.
Joint and Muscle Discomfort: Rapid muscle growth can outpace connective tissue adaptation, leading to joint stiffness and localized muscle pain, particularly in early cycles.
Absolute Contraindications
- Active or recent malignancy of any kind
- Known hypersensitivity to IGF-1 or analogs
- Pregnancy or breastfeeding
- Pediatric use (except in specific FDA-approved indications for growth hormone deficiency)
Relative Contraindications (Requires Enhanced Monitoring)
- Diabetes or significant insulin resistance
- Pre-diabetic metabolic profile
- Family history of cancer
- Cardiovascular disease
- Concurrent use of insulin or insulin-sensitizing medications
IGF-1 LR3 vs. Comparable Peptides
Understanding where IGF-1 LR3 fits in the broader peptide landscape helps set realistic expectations. Our full peptide comparison guide for 2026 covers this in depth, but here’s how the key compounds stack up mechanistically:
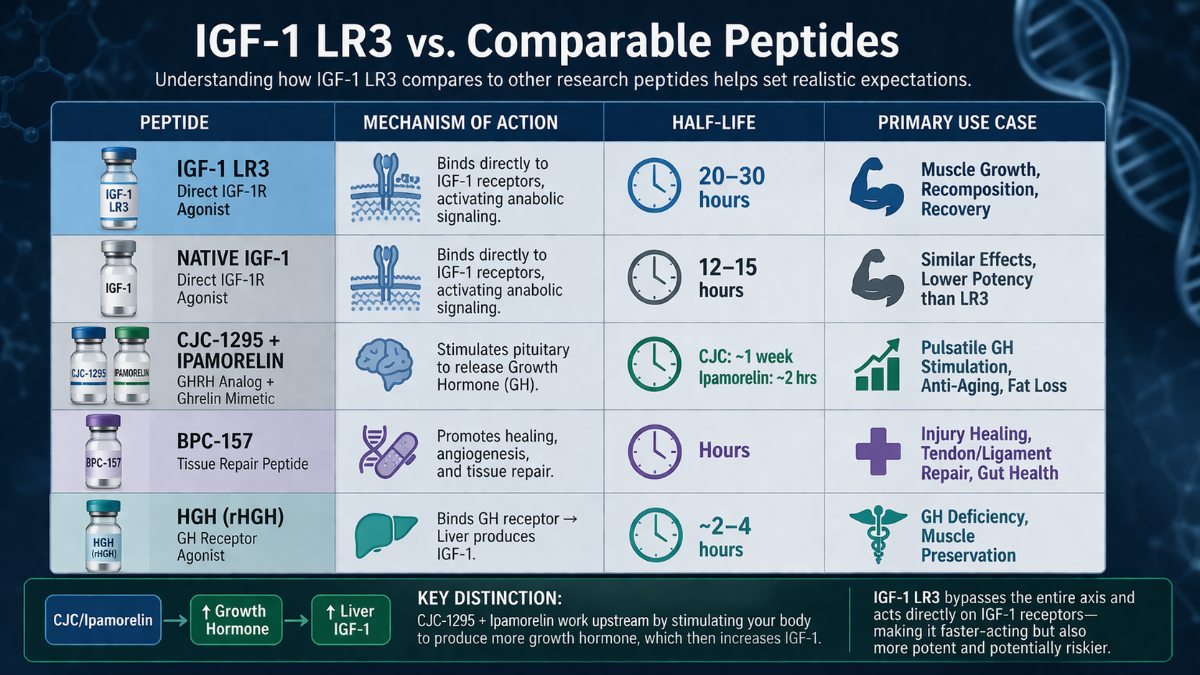
| Peptide | Mechanism | Half-Life | Primary Use Case |
|---|---|---|---|
| IGF-1 LR3 | Direct IGF-1R agonist | 20–30 hours | Muscle growth, recomposition, recovery |
| Native IGF-1 | Direct IGF-1R agonist | 12–15 hours | Similar effects, lower potency |
| CJC-1295 + Ipamorelin | GHRH analog + ghrelin mimetic → GH release | CJC ~1 week / Ipamorelin ~2 hrs | Pulsatile GH stimulation, anti-aging, fat loss |
| BPC-157 | Direct tissue repair | Hours | Injury healing, gut repair |
| HGH (rHGH) | GH receptor agonist → liver IGF-1 production | ~2–4 hours | GH deficiency, muscle preservation |
The CJC-1295 + Ipamorelin blend 10mg works upstream it stimulates the pituitary to release more growth hormone, which then stimulates the liver to produce more IGF-1. IGF-1 LR3 bypasses this entire axis and acts directly on tissue receptors. This makes it faster-acting but also more potent and riskier than GH secretagogue stacks.
For researchers focused on muscle development, the best peptide for muscle growth breakdown compares IGF-1 LR3 head-to-head with CJC-1295/Ipamorelin, Follistatin-344, and IGF-1 DES across mechanisms, half-lives, and research applications.
Why Purity Matters With IGF-1 LR3
Unlike many research compounds, IGF-1 LR3 1mg has a narrow therapeutic window the gap between an effective dose and one that causes hypoglycemia or other adverse effects is not wide. This makes purity and accurate concentration absolutely critical. An impure or underdosed product creates two distinct problems: ineffective research outcomes and unpredictable safety profiles. A vial labeled at 1mg that contains 0.6mg may seem like a minor discrepancy, but at 50 mcg/day, it represents a significant and uncontrolled dosing error.
Ageless Vitality Peptides applies the same quality standards to every compound in our catalog:
- ≥99% purity verified by HPLC and Mass Spectrometry
- Batch-specific Certificates of Analysis (COAs) are publicly available
- USA manufacturing in cGMP and ISO-certified facilities
- Third-party testing is independent of internal quality control
Learn more about our standards on the About Us page or review current product availability in the full research peptide shop.
IGF-1 LR3 Before and After: Key Results & Final Takeaways
- The science is real. IGF-1 LR3 acts through well-characterized molecular pathways (PI3K/Akt/mTOR) with documented effects on muscle growth, fat metabolism, tissue repair, and recovery.
- The timeline is gradual. Cellular effects begin immediately, subjective changes appear in 1–2 weeks, and measurable body-composition shifts develop over 4–8 weeks during a properly structured cycle.
- Cycling is pharmacologically necessary, not optional. Receptor downregulation after 4–6 weeks is well-documented. Continuous use increases risk without proportional benefit.
- Medical supervision is essential. Hypoglycemia risk is real and acute. Cancer contraindications are absolute. Individual metabolic variation is significant.
- Realistic expectations matter. Well-designed research protocols produce meaningful improvements in lean mass, recovery, and body composition not overnight transformations.
- The regulatory landscape is clear. IGF-1 LR3 is not FDA-approved for general use, is banned in sports, and is used experimentally in supervised clinical and research settings.
- Purity determines safety. Source only from manufacturers with verifiable third-party COAs and confirmed ≥99% purity our quality standards are publicly documented and independently verifiable.
Frequently Asked Questions
How long does IGF-1 LR3 take to work?
Cellular-level effects begin within hours of administration. Subjective improvements in recovery are typically noticeable within 3–14 days. Measurable body composition changes generally appear by weeks 2–4. Peak effects occur in the weeks 4–6 window of a cycle.
Is IGF-1 LR3 safe?
Under medical supervision, with proper dosing, cycling, and monitoring, the risk profile is considered manageable by practitioners in the peptide therapy and anti-aging medicine space. Unsupervised self-administration is considered high-risk by the medical community. It is not FDA-approved for general use, and long-term safety data remain limited.
What results can I realistically expect from IGF-1 LR3?
Realistic expectations from a supervised 4–6 week cycle with optimized training and nutrition: improved muscle fullness and vascularity, enhanced recovery between sessions, modest but measurable lean mass gains, potential body fat reduction, particularly in insulin-sensitive depots. The dramatic transformations in some before-and-after photos typically reflect multiple cycles, optimized supplementation, and, sometimes, concurrent use of other compounds.
How does IGF-1 LR3 compare to HGH?
IGF-1 LR3 acts more directly and specifically on tissue IGF-1 receptors, producing faster anabolic effects. HGH works indirectly it stimulates liver IGF-1 production and has broader metabolic effects. Some anti-aging protocols combine both. IGF-1 LR3 is not a substitute for HGH and vice versa; they have distinct mechanisms and use cases.
Can IGF-1 LR3 cause cancer?
No direct causal link has been established in research. However, because IGF-1 signaling is involved in cellular proliferation pathways implicated in oncogenesis, existing or precancerous conditions are considered absolute contraindications. Individuals at elevated cancer risk should not use IGF-1 LR3. Ongoing monitoring is essential in any supervised protocol.
What is the standard IGF-1 LR3 dosage for research?
Most research protocols use 50–100 mcg per day administered subcutaneously, with study durations of 4–6 weeks. Clinical supervised protocols typically individualize dosing based on metabolic profile, body composition, and treatment goals. Use our Peptide Calculator to convert your target mcg dose into precise reconstitution volumes.
Does IGF-1 LR3 require PCT (Post-Cycle Therapy)?
IGF-1 LR3 does not suppress testosterone production as anabolic steroids do. However, it does suppress endogenous IGF-1 signaling and affects the GH axis. Some practitioners recommend light PCT protocols using GH secretagogues to maintain GH axis activity during the off period. The CJC-1295/Ipamorelin combination is a commonly researched option for this purpose.
Where can I source research-grade IGF-1 LR3?
Purity is everything with IGF-1 LR3. An under dosed or contaminated product carries significant safety risks. Ageless Vitality Peptides is manufactured in the USA, achieves ≥99% purity verified through HPLC and Mass Spectrometry, and provides batch-specific Certificates of Analysis. Browse the full research peptide shop or visit the homepage to review quality standards and current product availability.









{kind=link}
{kind=link}